

Lymphedema is a chronic disorder of the lymphatic system characterized by abnormal accumulation of lymph in tissues, leading to progressive, persistent, and sometimes disabling swelling of a limb or body region. Unlike simple transient edema, lymphedema is a structural disease caused by insufficient lymphatic transport. It is not just excess water—the accumulated fluid is rich in proteins, which explains the inflammatory and fibrotic changes that develop over time.
This condition can affect the lower limbs, upper limbs, genital region, trunk, and, more rarely, the face. It can appear at birth or develop secondarily following a medical event, most often surgery with lymph node dissection or radiotherapy.
The Lymphatic System: Essential but Fragile
The lymphatic system is a parallel network to the venous system. It collects interstitial fluid between cells, filters it through lymph nodes, and returns it to the bloodstream. It plays a major role in immunity, fluid regulation, and intestinal fat absorption.
Every day, several liters of interstitial fluid must be recovered by lymphatic capillaries. When the system functions poorly—either due to congenital abnormalities or secondary damage—transport capacity becomes insufficient, and lymph accumulates in the tissues.
This stagnation gradually causes:
- Chronic inflammation
- Activation of fibroblasts
- Skin thickening
- Local adipose tissue increase
- Impaired local immunity
Thus, untreated lymphedema is a progressive disease.
Primary and Secondary Lymphedema
Primary lymphedema results from a congenital abnormality of the lymphatic system. Vessels may be absent, too few, or malformed. It can appear at birth, during adolescence, or later in adulthood.
Secondary lymphedema, much more common, develops after an acquired lymphatic injury. Main causes include:
- Surgery with lymph node removal
- Radiotherapy
- Severe trauma
- Chronic infections
- Morbid obesity
- Compressive tumors
- Filariasis in tropical regions
In developed countries, the most frequent cause is cancer treatment, particularly breast or pelvic cancers.
How Lymphedema Manifests
Early symptoms are often subtle. Patients may describe heaviness, unusual tightness in a limb, or swelling at the end of the day. Shoes become tight, and rings no longer fit.
Gradually, the swelling becomes permanent. In the initial stage, finger pressure leaves an indentation (pitting sign). Over time, tissues become firm, fibrotic, and thickened, and the skin may change, becoming dry, thick, or even verrucous in advanced stages.
Recurrent skin infections are common. Erysipelas is a classic, sometimes recurring complication that further worsens lymphatic dysfunction.
Stages of Lymphedema
Lymphedema is a dynamic disease that develops progressively over years, not abruptly. Understanding these stages is essential, as treatment potential and options vary depending on when management begins.
Progression is driven by chronic accumulation of protein-rich lymph in tissues, triggering a local inflammatory cascade. Macrophages are activated, fibroblasts produce collagen, adipose tissue proliferates, and the skin structure gradually changes. The longer the disease progresses, the more irreversible the structural changes.
Traditionally, four clinical stages are distinguished:
- Stage 0: Latent or subclinical
- Stage I: Spontaneously reversible
- Stage II: Spontaneously irreversible
- Stage III: Elephantiasis
Stage 0: The Silent Stage (Latent)
Stage 0 is often unrecognized because no visible swelling exists. Nevertheless, the lymphatic system is already compromised, with reduced transport capacity that remains adequate at rest. This stage can last months or years.
Patients may notice subtle signs: heaviness, intermittent tightness, unusual fatigue in a limb, or a sense of swelling at the end of the day. Standard clinical exams may appear normal, with limb circumferences within the usual range.
Specialized tests such as lymphoscintigraphy or indocyanine green (ICG) fluorescence imaging may reveal slowed lymph flow or areas of stasis.
This stage is particularly common after lymph node dissection for breast or pelvic cancer. The lymphatic system is functioning at “reduced reserve,” and trauma, infection, or weight gain can trigger clinical lymphedema.
Early intervention at this stage is crucial to prevent the onset of visible swelling.
Stage I: Reversible Stage
At stage I, swelling becomes visible. It is typically soft, with a clear pitting sign. Edema fluctuates throughout the day and decreases with limb elevation or overnight rest.
Fluid is the predominant component, and tissues are not yet significantly remodeled. Fibrosis is minimal or absent.
Clinical features include:
- Gradual swelling during the day
- Improvement in the morning
- Tension or tightness
- Occasional mild functional discomfort
Skin remains supple and normal in appearance.
Stage I is considered the most favorable for intervention. Manual lymphatic drainage combined with appropriate compression often achieves significant volume reduction. With proper treatment and strict adherence, progression to advanced stages can be avoided.
Stage II: Spontaneously Irreversible Stage
Stage II is characterized by permanent edema that no longer resolves completely at rest. The fluid component diminishes as fibrotic and adipose tissue accumulates.
Changes include:
- Fibroblast proliferation
- Excess collagen deposition
- Adipose tissue hypertrophy
- Chronic inflammation
The limb becomes heavier and less flexible, and mobility may be limited. Skin infections become more frequent due to impaired local immunity.
Conservative treatment remains essential but yields slower and partial results. Surgical evaluation may be considered depending on the condition of the lymphatic collectors.
Stage III: Elephantiasis
Stage III represents the most advanced form, with significant structural changes and massive volume increase.
Characteristic skin changes:
- Severe thickening
- Hyperkeratosis
- Papillomatosis
- Verrucous changes
- Deep skin folds
- Possible exudates
Fibrosis is intense, tissue is hard and sometimes painful, and limb deformities are common. Infections are frequent and may be severe.
In this stage, adipose and fibrotic components predominate over fluid. Simple drainage is insufficient, and specialized surgical procedures such as lymphedema-specific liposuction or combined approaches may be required.
Underlying Biological Progression
Molecular changes occur early, including:
- Cytokine activation
- Extracellular matrix remodeling
- Abnormal angiogenesis
- Lymphatic stasis-induced adipogenesis
The longer the disease persists, the more structural “fixation” occurs, highlighting the importance of early intervention.
Factors Accelerating Progression
- Recurrent infections
- Obesity
- Prolonged immobility
- Local trauma
- Lack of compression
- Chronic heat exposure
Weight gain is particularly harmful, as excess adipose tissue adds pressure to lymphatic collectors.
Why Early Treatment Matters
In stages 0 and I, the lymphatic network retains some functionality. Conservative and microsurgical techniques have higher effectiveness.
Stage II results are possible but more limited, while stage III focuses on volume reduction and complication prevention rather than restoring normal function.
Key components:
- Early detection
- Regular monitoring of at-risk patients
- Patient education
- Stage-appropriate specialized intervention
Lymphedema vs Lipedema: A Critical Distinction
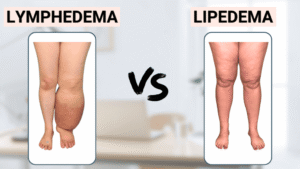
It is essential to differentiate lymphedema from lipedema, as the mechanisms are entirely different.
Lipedema:
- Chronic adipose disorder
- Predominantly in women
- Symmetrical fat accumulation in lower limbs (sometimes upper)
- Feet usually spared (“cuff sign”)
- Pressure does not leave persistent indentation
- Pain on palpation
- Easy bruising
- Often resistant to dieting
Lymphedema:
- Can be unilateral
- Often affects hands or feet
- Progresses to fibrosis
- Associated with recurrent infections
Mixed forms, called lipo-lymphedema, also exist. Clinical exam, disease history, and imaging are essential for differentiation.
Diagnosis
Diagnosis is mainly clinical, but modern imaging plays a key role in treatment planning:
- Doppler ultrasound (to exclude venous causes)
- Lymphoscintigraphy
- MR lymphangiography
- Indocyanine green imaging
These tests visualize the lymphatic network, assess collector patency, and identify obstructions.
Possible Complications
Untreated lymphedema may lead to:
- Recurrent skin infections
- Severe fibrosis
- Elephantiasis
- Major functional impairment
- Psychological distress
Rarely, lymphangiosarcoma can occur after decades of disease.
Conservative Treatment: The Essential Foundation
Initial management relies on intensive conservative therapy, including:
- Manual lymphatic drainage
- Multilayer bandaging
- Proper elastic compression
- Targeted exercises
- Rigorous skin care
This “decongestive” phase reduces limb volume. Maintenance is lifelong. Compression is a cornerstone, not a mere accessory.
Lymphedema Surgery: When and Why
Surgery is not first-line. It is considered when intensive conservative therapy fails or disease progresses.
Modern microsurgery and advanced lymphatic imaging have made surgical intervention a viable, effective option in selected patients.
Surgical goals may include:
- Restoring functional lymphatic drainage
- Diverting lymph to the venous system
- Reconstructing deficient lymphatic networks
- Removing irreversibly altered tissues
Choice depends on disease stage, quality of remaining lymphatic collectors, and the ratio of fluid to fibrofatty tissue.
Preoperative Evaluation
Precise lymphatic mapping is essential. Clinical examination alone is insufficient. Common assessments include:
- Lymphoscintigraphy
- MR lymphangiography
- ICG fluorescence imaging
- High-resolution ultrasound
This determines if functional lymphatic vessels remain, which is crucial for physiological techniques.
Lymphaticovenular Anastomoses (LVA)
LVA connects functional lymphatic vessels (sometimes <0.5 mm) to small superficial veins, bypassing obstructions. This super-microsurgical procedure is minimally invasive, with short hospitalization and rapid recovery. Most effective in early-stage fluid-predominant lymphedema.
Vascularized Lymph Node Transfer (VLNT)
VLNT transplants functional lymph nodes with their vascular pedicle from donor sites (e.g., groin or supraclavicular) to the affected limb, promoting neo-lymphangiogenesis and establishing new drainage centers. Indicated for moderate-to-advanced lymphedema when LVA is not feasible. Results develop gradually over months.
Specialized Lymphedema Liposuction
In late stage II and stage III, swelling is due to fibrofatty tissue accumulation. Specialized liposuction selectively removes hypertrophied tissue under tourniquet. Permanent compression postoperatively is required.
Combined Techniques
- LVA + VLNT
- VLNT + liposuction
- Early LVA + secondary reductive procedure
Treatment plans must be individualized.
Indications for Surgery
Surgery is considered when:
- Intensive conservative therapy has been followed
- Swelling remains significantly disabling
- Recurrent infections occur
- Quality of life is impaired
- Imaging shows favorable anatomy
Contraindicated in patients non-compliant with therapy, purely venous edema, or absence of functional lymphatic structures.
Expected Benefits
- Significant volume reduction
- Fewer infections
- Improved mobility
- Reduced dependency on compression
- Enhanced quality of life
Patient selection is critical. Outcomes depend on disease duration and severity.
Lymphedema and Quality of Life
Beyond swelling, lymphedema deeply impacts daily life: clothing difficulties, infection fears, permanent compression, and self-esteem. Psychological support may be needed.
Conclusion
Lymphedema is a complex chronic disease requiring early diagnosis and specialized management. It is not merely swelling or an aesthetic concern but a progressive structural disorder. Differentiation from lipedema is essential to avoid treatment errors. Each case must be evaluated through thorough clinical and imaging assessment.
In Tunisia, advanced lymphedema management requires mastery of both intensive conservative techniques and modern microsurgical procedures. Currently, only Dr. Ramy Ben Salah and Dr. Youssef Gam possess comprehensive expertise to effectively treat all forms of lymphedema, including complex and advanced cases.
Specialized evaluation remains essential to establish a personalized treatment plan and optimize long-term outcomes.